
Root Fracture Treatment & Intentional Replantation|Takahashi Dental Clinic, Minoh-Osaka
We specialize in microscope-assisted adhesive restoration and intentional replantation for root fractures and advanced caries.
Learn more on our dedicated specialty site: rootfracture.com.
Hello — we are Takahashi Dental Clinic in Minoh, Osaka.
Even for teeth that have been told “extraction is necessary” due to root fracture or advanced caries, we aim to preserve them as much as reasonably possible.
The videos below explain our actual treatment methods and cases in an easy-to-understand manner—please take a look.
① Teeth Eligible for Repair at Our Root-Fracture Specialty (Cases for Intentional Replantation & Adhesive Restoration)
● Root-Fracture Specialty: Teeth That May Be Saved with Intentional Replantation & Adhesive Restoration【Takahashi Dental Clinic】
Even teeth considered “hopeless—must extract” at other clinics can sometimes be treated at our clinic using intentional replantation or adhesive restoration.
In this video, we present various photos of root fractures so you can compare them with your own condition.
Before giving up, please feel free to consult us.
② Case: Intentional Replantation & Extraoral Adhesive Repair of a Lower Premolar
● Don’t Give Up Even with Dark Discoloration & Root Fracture! Saving a Lower Premolar via Intentional Replantation & Adhesive Repair
This tooth had turned dark due to caries and the root had snapped midway. We treated it using “intentional replantation,” temporarily extracting the tooth for repair and then returning it to its socket.
It’s a real case of a patient who had been told to extract the tooth everywhere and felt at a loss.
We explain the flow and key points of advanced root-fracture treatment.
Our Specialized Approach to Root-Fracture Care, Cysts, and Caries
“Specialized in repairing and replanting fractured roots and advanced caries — Takahashi Dental Clinic, Minoh-Osaka.”
Root-Fracture Treatment Methods and Esthetic Recovery
Our videos introduce concrete cases requiring adhesive repair or intentional replantation—for example, “a tooth split in two,” “root cracks,” and “root fractures,” with explanations of treatment methods.
Even when root canal therapy alone cannot resolve the issue, we can address apical cysts, fistulas, and periapical lesions.
Some patients diagnosed with “vertical root fracture” are advised to extract and proceed with implants or bridges. Our goal, however, is to preserve teeth whenever feasible to restore a natural and beautiful smile.
If you have problems such as bad breath or swollen gums after leaving a bad tooth for over a year, please consult us with confidence.
③ Adhesive Repair Case (Lower Molar Split Completely Down to the Root)
● Saving a Molar that Split to the Root Detected Early! Adhesive Repair Completed Before Infection
This lower molar had freshly split completely in two.
Because treatment was done before infection developed, we could complete care with adhesive restoration without surgery.
Once time passes and pus appears, surgery is more likely to be necessary—this video explains the importance of early visits.
④ Adhesive Repair Case (A Ceramic Crown Fell Off and Caries Progressed Underneath)
● Caries Progressing Under a Ceramic Crown… Can We Still Save It? Avoiding Extraction with Advanced Adhesive Restoration
A ceramic crown suddenly came off, and the internal tooth had severely collapsed—another clinic said even placing a core would be impossible.
However, because the root portion was stable, we restored it with time-intensive, high-precision adhesive techniques.
We explain key points for avoiding extraction.
Specialized Care that Restores Hope
After root canal therapy or surgical procedures at other clinics, patients are sometimes still told “extraction is necessary,” and even if they wish to avoid extraction, they may be recommended implants.
At university hospitals, some patients are advised to extract because “there’s a crack in the root,” which can feel devastating. At our clinic, through specialized care and case videos, we try to offer new hope.
By visiting us, you may gain an opportunity to reconsider the necessity of extraction.
Conservative Care for Root Fractures: A Future-Oriented Approach
In the past, I worked in a hospital oral & maxillofacial surgery department, performing tongue-cancer and maxillofacial fracture surgeries. We also received many difficult cases (such as wisdom tooth extraction) referred by private practices.
However, there were cases where I questioned whether extraction was truly necessary. I wondered if root canal therapy might allow the tooth to be preserved—and on examining extracted teeth, I often found substantial healthy tooth structure remained.
While hospital OMS mainly handles requests from referring dentists, as a private practitioner now I actively perform tooth-preserving therapy for teeth that were diagnosed as “need extraction.”
For teeth indicated for extraction—residual roots and root fractures—we employ adhesive restoration and intentional replantation. Our goal is not only to save the tooth, but also to improve inflammation control, occlusal function, and esthetics.
Even if a tooth is cracked or fractured, many patients wish to keep it and place a crown. We focus on treatments that maintain both health and esthetics for the long term.
Tooth-Preserving Care: Avoiding Extraction at Our Clinic
Extracting a tooth and restoring with an implant, bridge, or denture is relatively straightforward, whereas preserving a tooth is more challenging and time-consuming.
Even dentists specializing in adhesive repair for root fractures may find some cases difficult; we respect patient preferences and pursue preservation as far as reasonably possible.
Our aim is to help you use your own teeth for as long as possible. From initial care to endodontic therapy, we follow a policy of minimizing pain and preserving tooth structure without unnecessary cutting or extraction, delivering careful and reassuring treatment.
Comprehensive Care Tailored to Patient Needs
Even in cases where extraction is typically recommended, we offer a variety of tooth-preserving options. For first-time visitors, we start by resolving the problem that bothers you the most.
Whether it’s tooth pain, ill-fitting dentures, lost fillings, repairs for dentures or crowns/bridges, chipped teeth, or bleeding gums—we first provide necessary urgent care and then move on to the next steps.
We explain not only your current oral condition but also potential future risks if nothing is done. We prioritize your wishes and never force treatment. We want you to choose a plan you truly accept.
Even if you have systemic conditions (e.g., heart disease) and were told treatment is difficult elsewhere, we collaborate with regional hospitals to fully consider systemic factors and treat caries and periodontal disease safely.

A case where a post-crown came off and extraction with implant or denture was suggested. Even if caries extends below the gumline, we can pursue tooth preservation as private treatment if the patient wishes.

Restored post-crown. We utilized the entire original root and placed a ceramic crown.

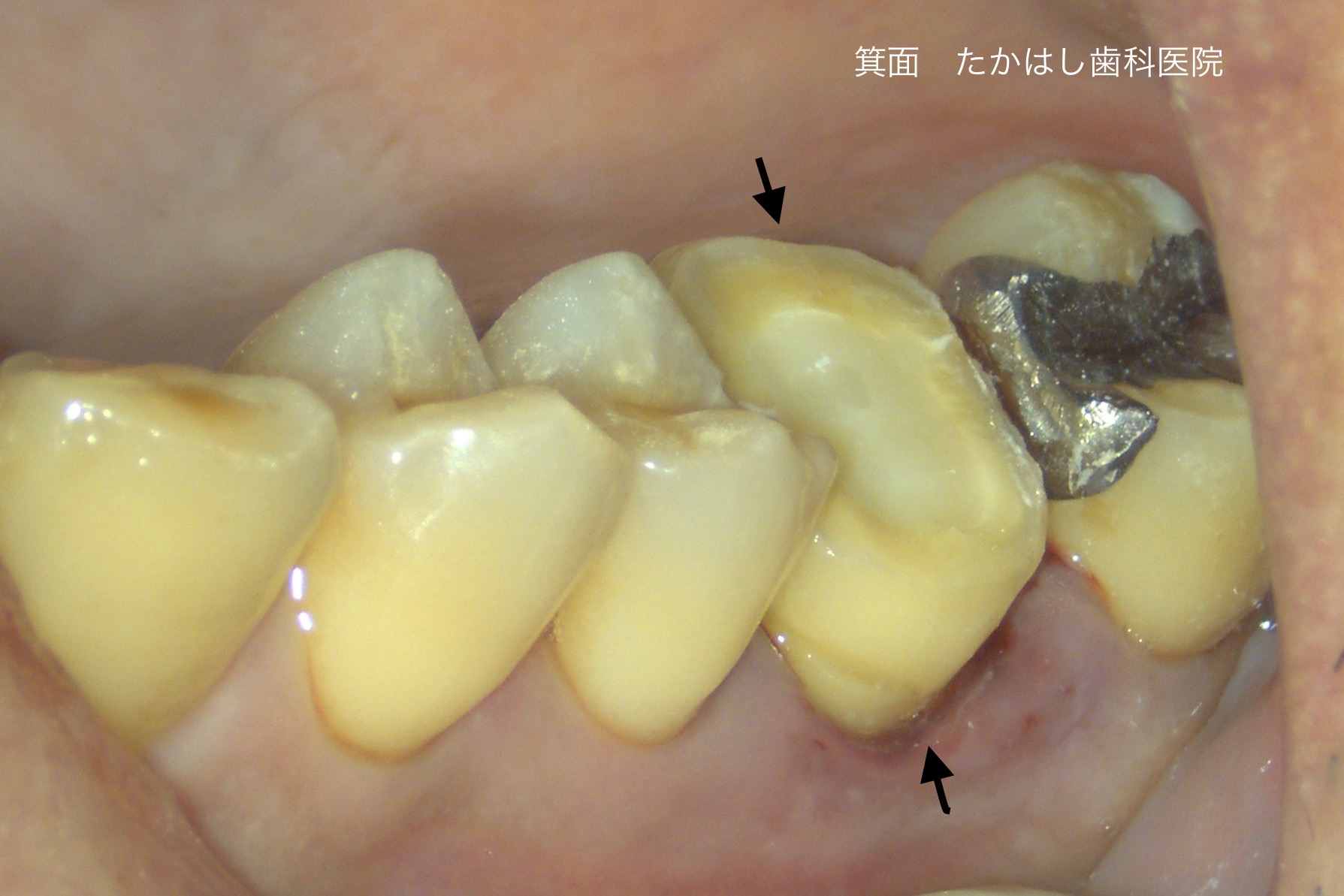
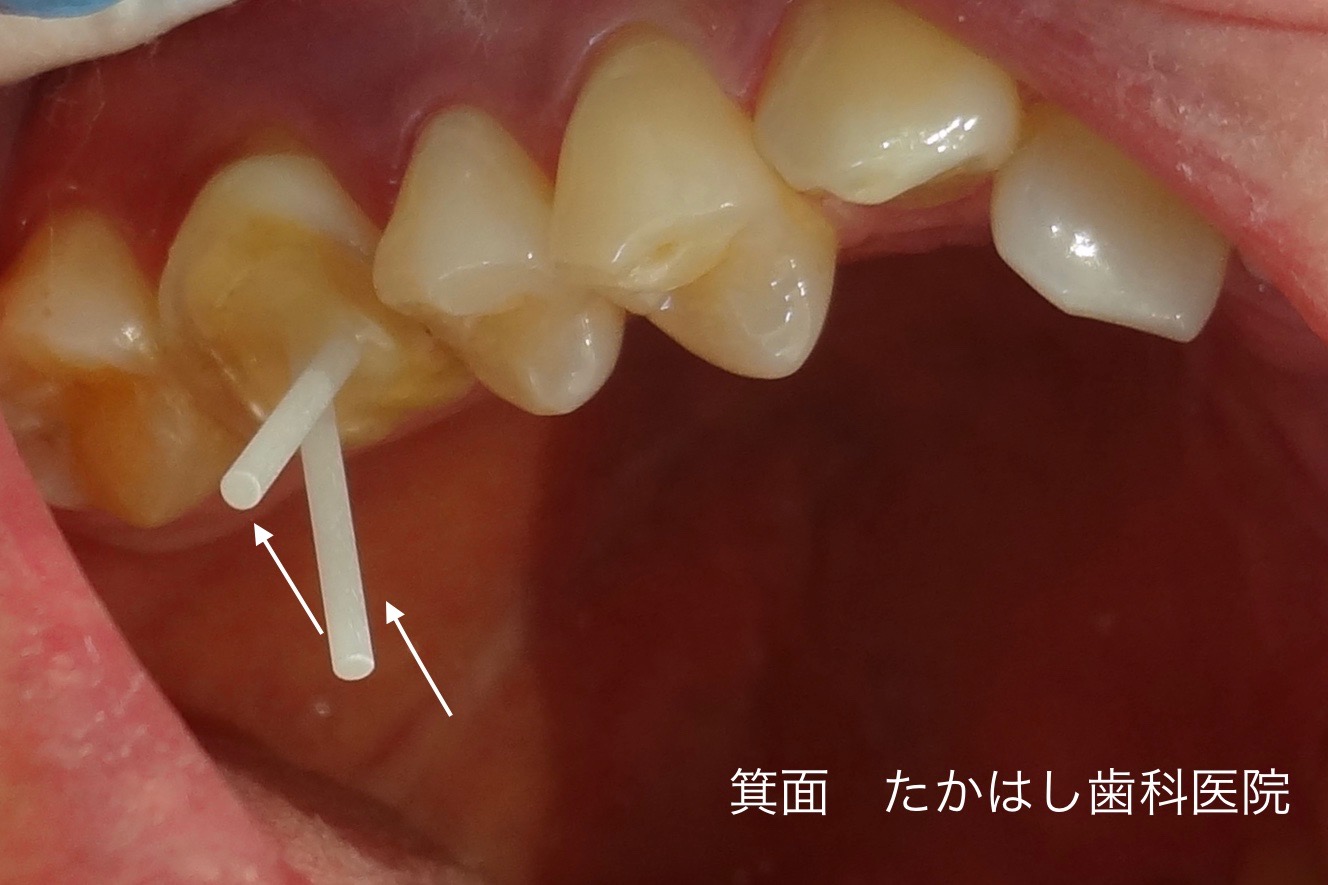
Advanced caries caused the tooth to fracture from the root, leaving the root submerged under the gum. The patient wished to “avoid extraction and keep the tooth.”

Immediate post-treatment photo after non-extraction caries care. As indicated by the arrows, two metal crowns were splinted to treat the posterior region.
The video above shows a case of treating extensively damaged caries.
Even for Fractured Teeth, We Aim to Save Them with Adhesive Repair and Intentional Replantation

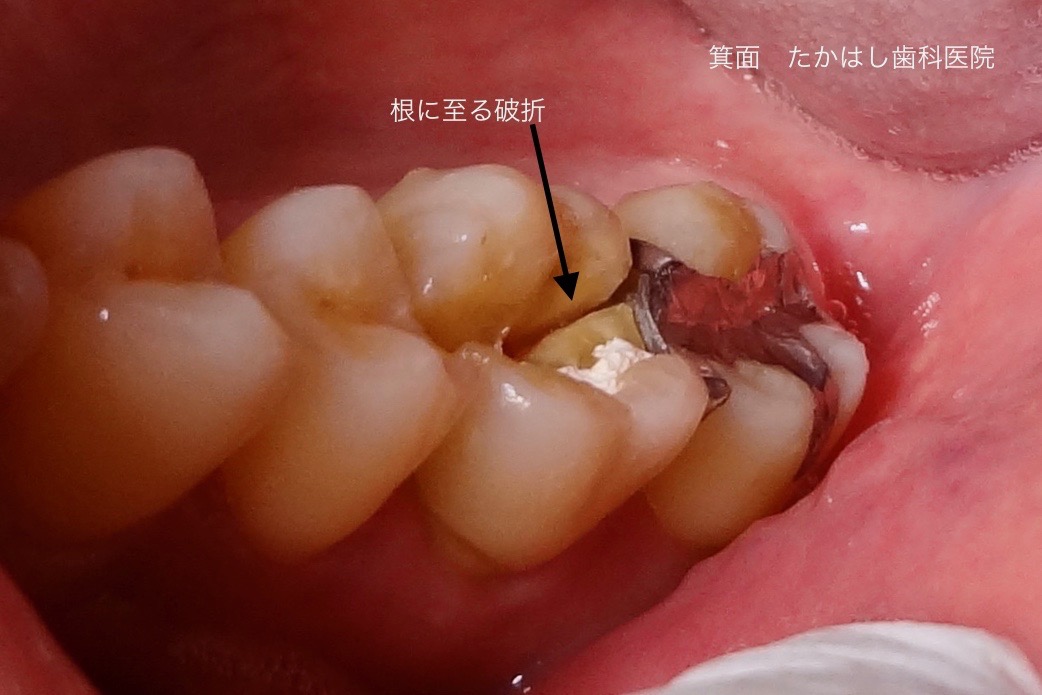
A crown fracture was observed in an upper molar. At the first visit the tooth was very mobile and hardly functional for chewing.
It often occurs when biting hard or resilient foods such as meat. Main symptoms include severe pain on biting, sensitivity, and mobility.
If left for months, infection can enter through the fracture line and the bone around the root may gradually resorb (bone loss).
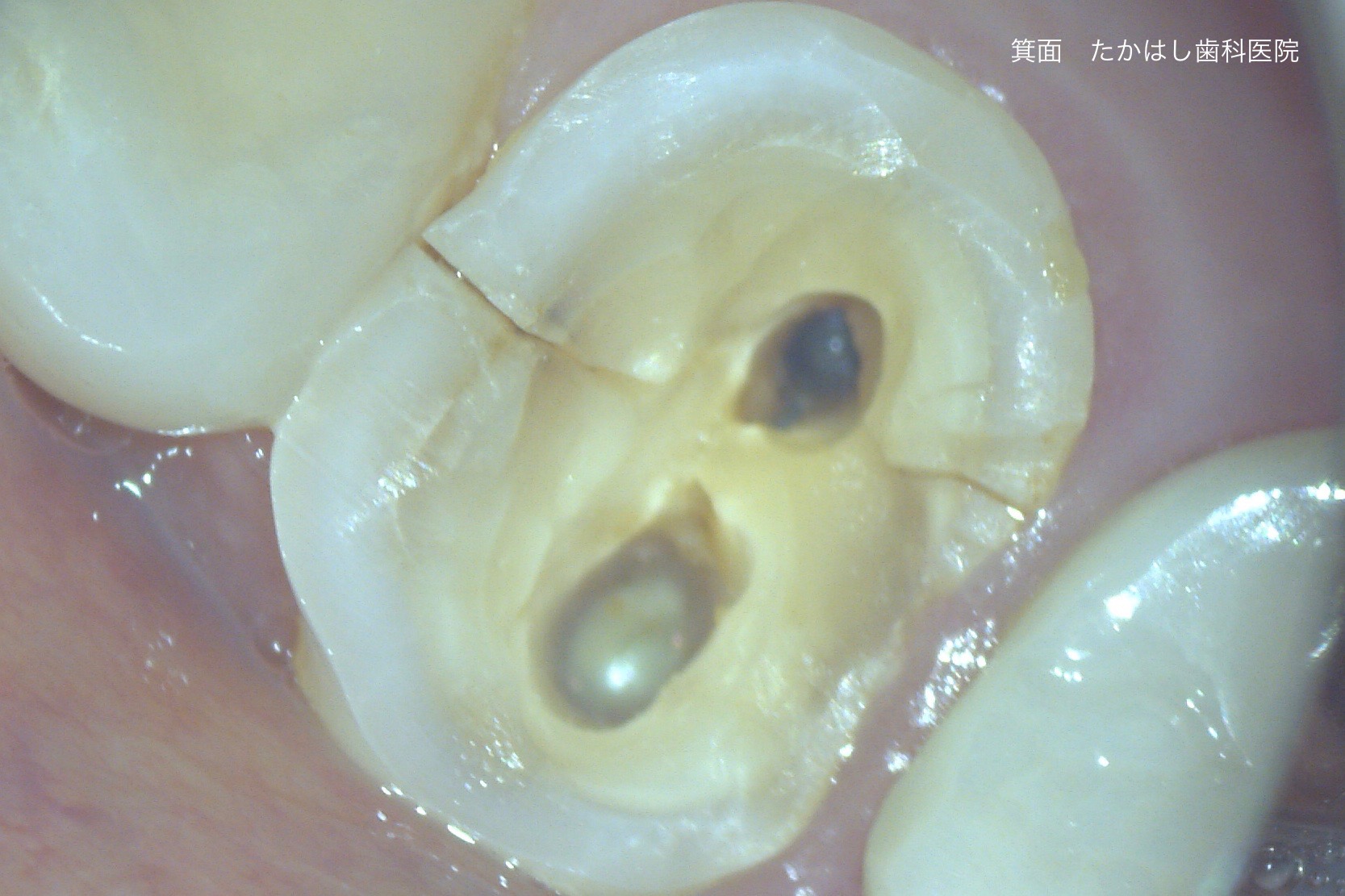
The photo above shows the intraoral view under a microscope. The fracture line reaches the pulp.
If treated while fresh, repositioning is easier and intraoral repair may be possible in many cases.
Assessing the Extent with CT and Microscope
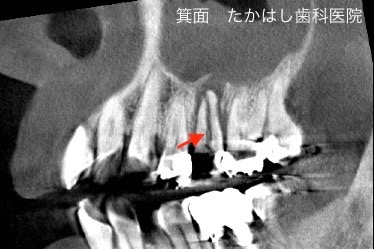
The CT image above shows the condition several months after the fracture. The root is split completely in two.
Repairing the root in this case requires an extraoral approach.
Case 1: Adhesive Repair & Intentional Replantation for Root Fracture
This is a typical example of a vertical root fracture of a posterior tooth—usually considered an indication for extraction.
Many patients are advised to have implants or bridges, but this patient visited us hoping to “keep my own tooth despite being advised to extract.”
Treatment steps: When the fracture extends to the root and segments are separated, an extraoral approach is required.
Under local anesthesia, we carefully extract the root and directly repair the split tooth. We also manage infected bone as needed.
Under the microscope we perform root repair, apicoectomy if needed, adhesive restoration, and fiber-reinforced core build-up.
After repair, the tooth (arrow) is repositioned and splinted. After about 3 months, we take impressions and proceed with a zirconia crown or equivalent.

Final state after placing a ceramic crown.
Upon request, even in cases diagnosed as crown-root fracture (private treatment), we proactively perform adhesive repair under the microscope.
After endodontic therapy, we reinforce the root with a glass-fiber post/core.
If intraoral repair is impossible, we consider surgical approaches such as apicoectomy, root resection, or intentional replantation.
Case 2: Adhesive Repair & Intentional Replantation for Root Fracture
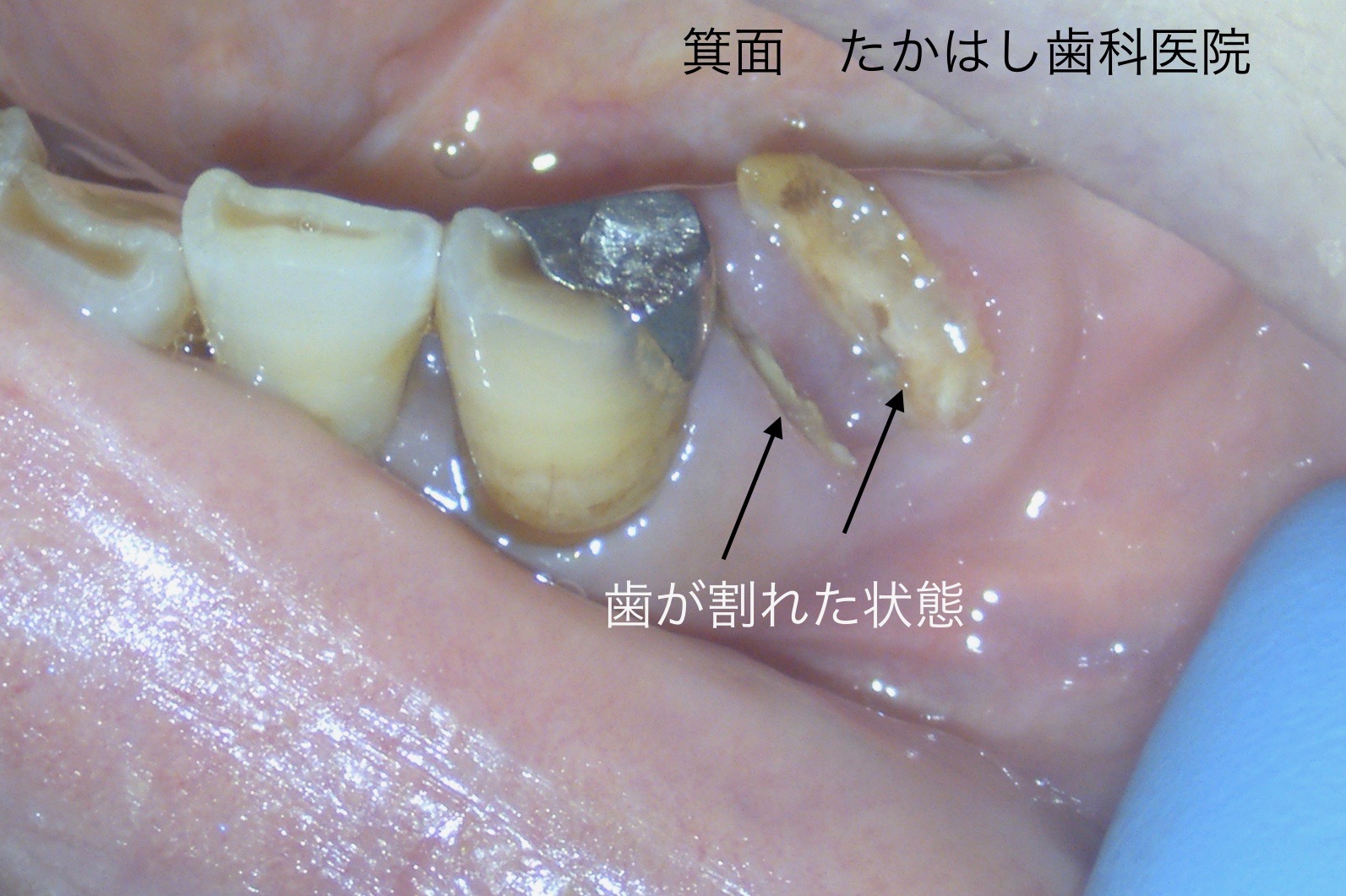
Case 2: The arrow indicates the fracture site of the lower left molar. Several months had passed and the root was sinking below the gumline.
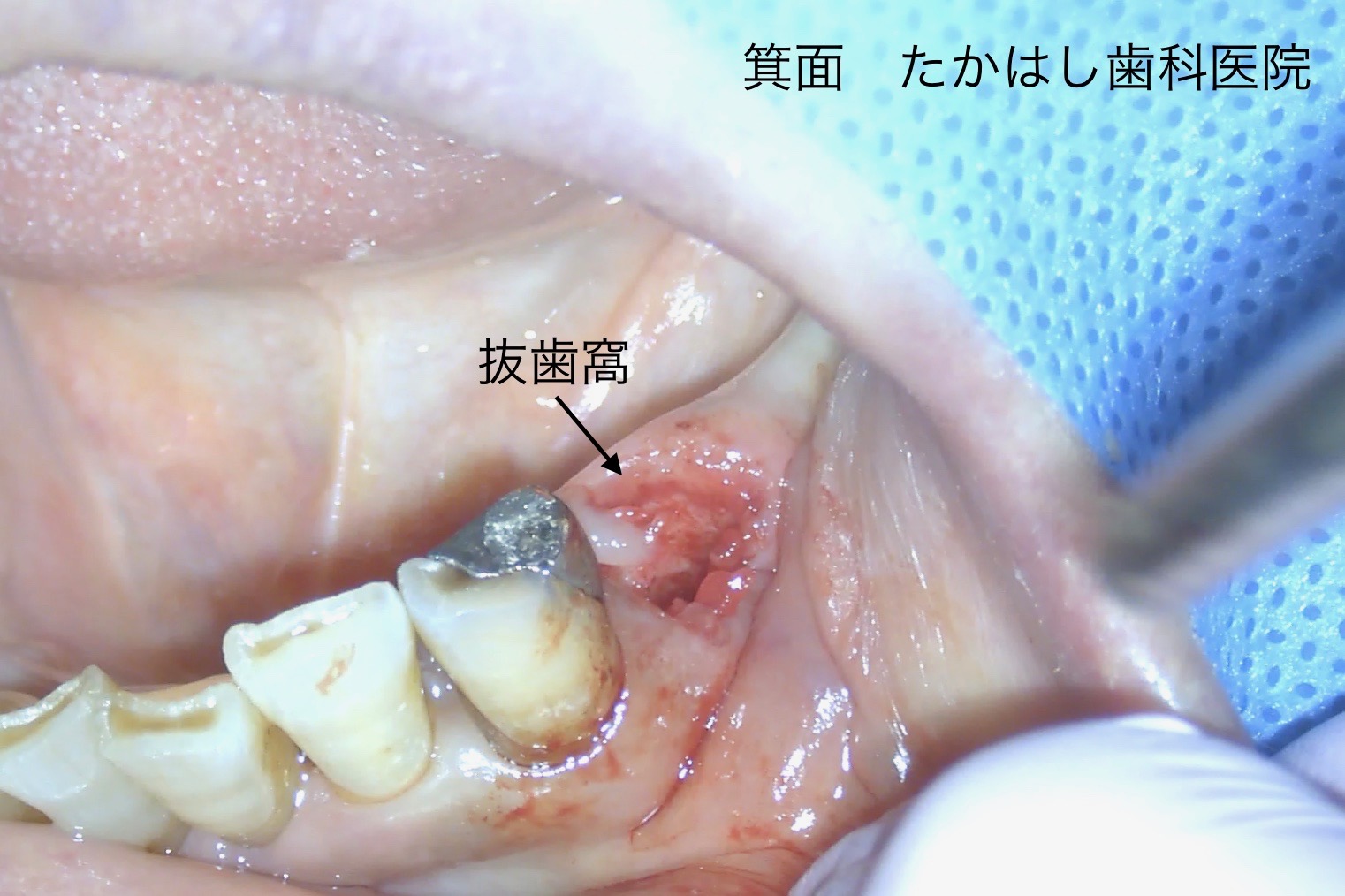
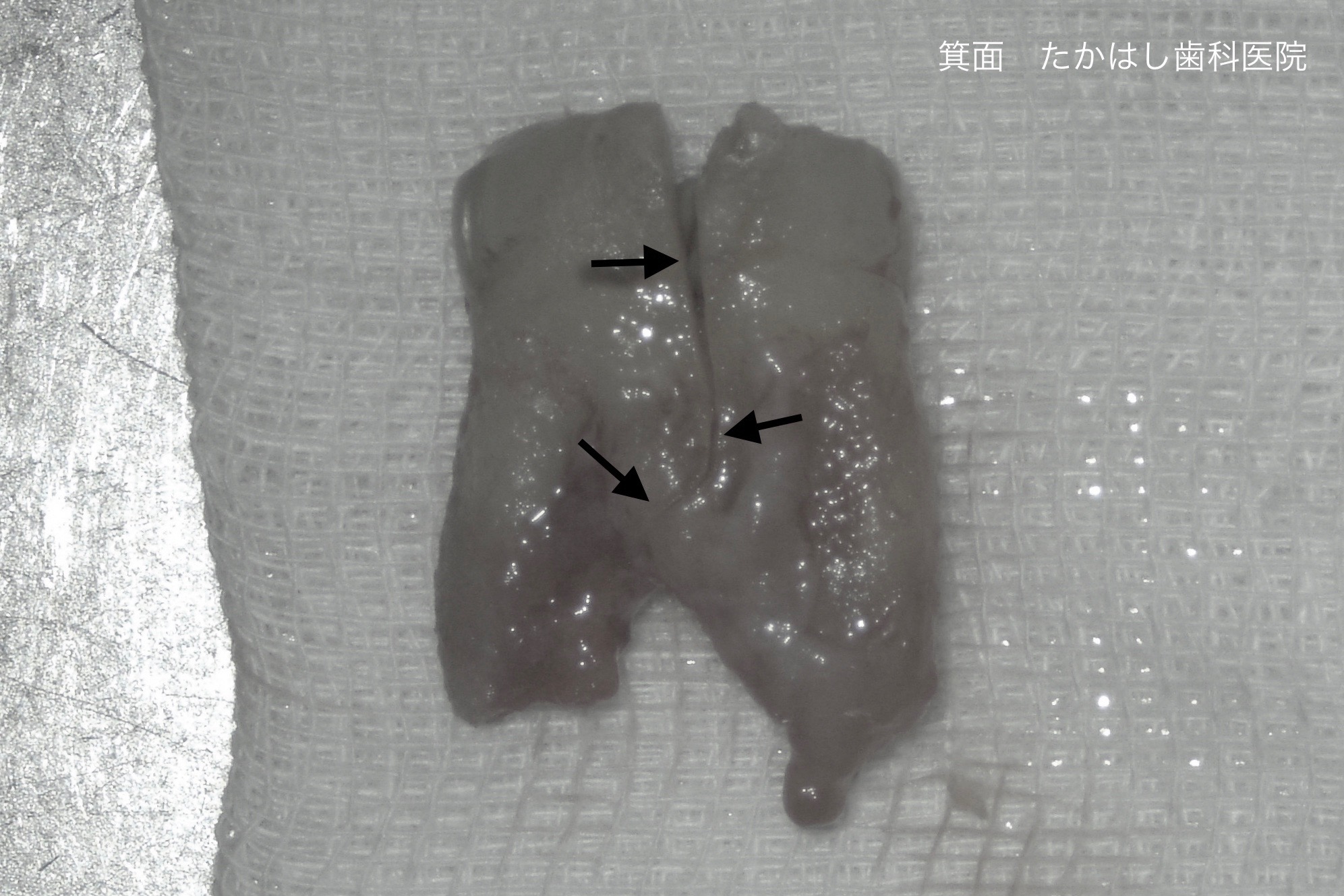
Because the fracture extended to the root, extraoral management was necessary. The arrow above shows the temporarily removed tooth. If the fracture does not split the root segments, intraoral repair may be possible.
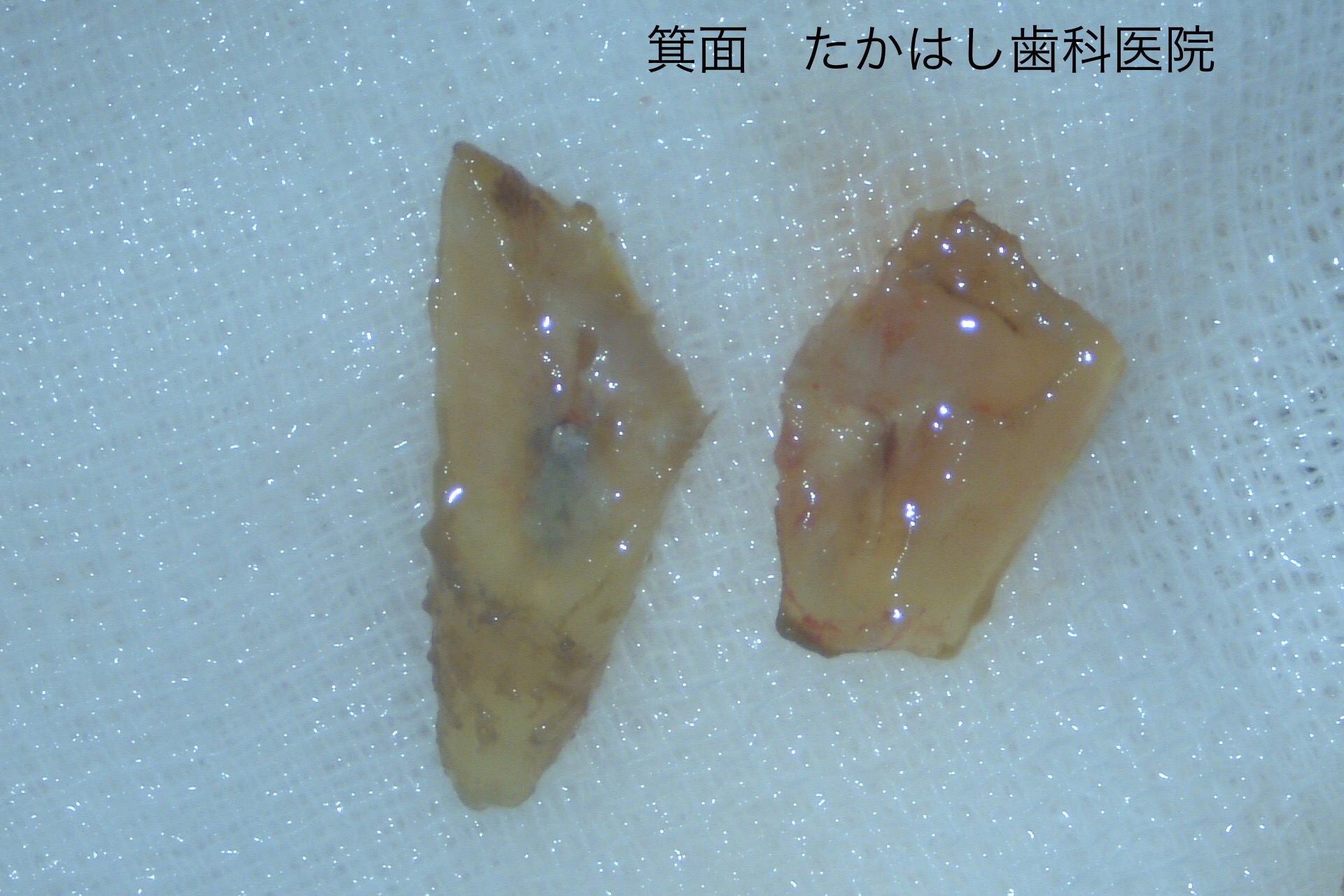
This shows the tooth after extraction. Although completely split, appropriate repair allowed us to rebuild the root.
Under the microscope, we repaired the fracture, performed endodontic therapy, and reinforced the core with fiber.
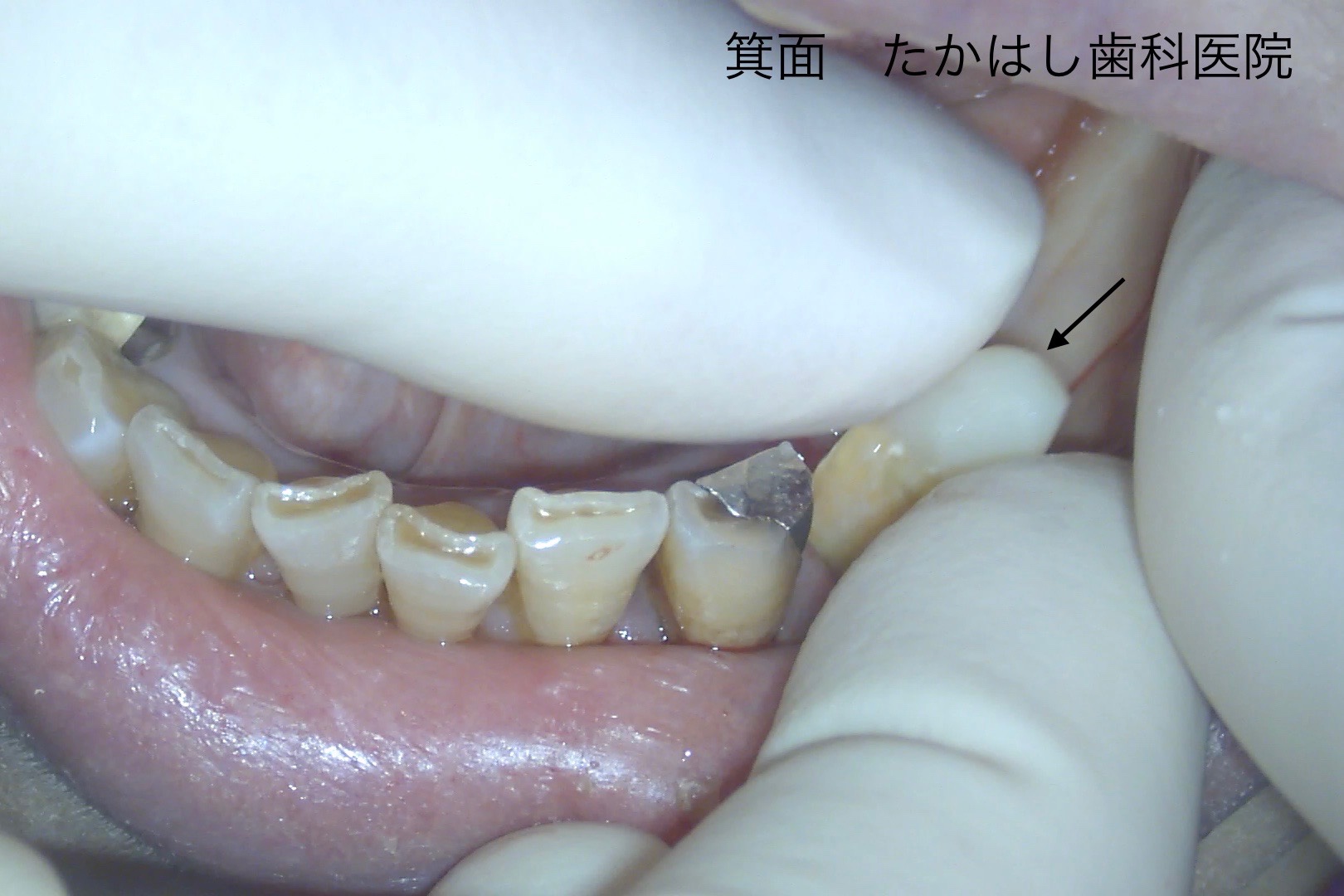
After repair and fiber-core build-up, the tooth was replanted in its original position.
We typically splint for about 2–3 months, then take impressions and fabricate the final crown for occlusal rehabilitation.

The adjacent metal crown was also replaced, and ceramic crowns were placed to complete treatment.
Case 3: Adhesive Repair (Intraoral Approach)

Case 3: The arrow indicates an upper posterior tooth. Post-crowned teeth without vital pulp tend to fracture more easily, but in this case the tooth had been healthy.
However, due to bruxism etc., the pulp (nerve/blood supply) had deteriorated—non-vital teeth can become “like dry wood” and fracture more easily.
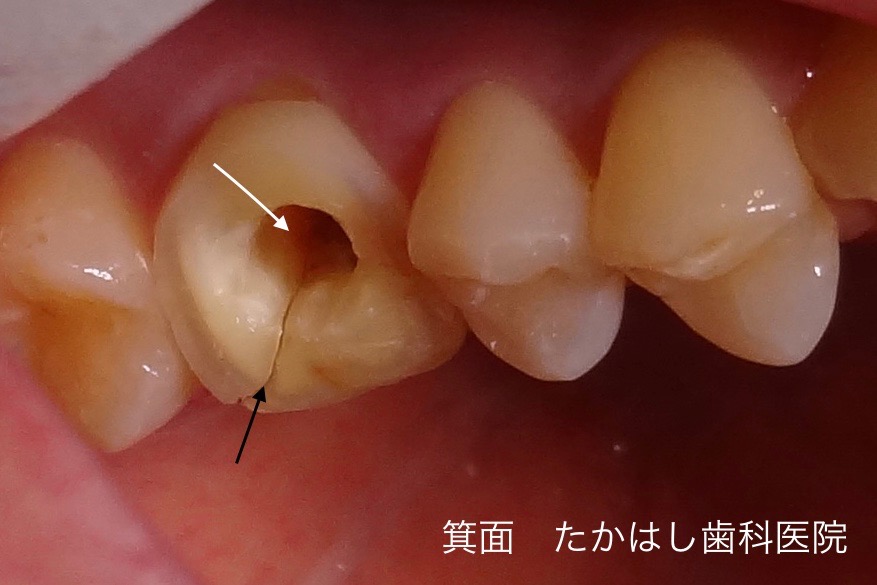
The fracture (black arrow) extended near the root, but intraoral repair alone was possible.
To treat the necrotic pulp we accessed through the center of the tooth (white arrow) for root-canal treatment and then repaired the fractured area.
Direct bonding with a glass-fiber core constructed.

Final restoration with a palladium-alloy crown.
Treating Residual Roots (I Don’t Want Extraction for an Implant!)

The photo above shows residual roots typically indicated for extraction. As private treatment, we actively pursue tooth-preserving options to avoid implants when feasible.
Private Case: Two Lower Left Molars Fractured and Declared for Extraction

The crown had detached after a root-level fracture. Because the caries extended below the gumline, extraction was recommended and the patient sought a second opinion.

This is the zirconia crown used to restore the fractured tooth. To utilize the remaining root, we operate under a microscope.
We preserve as much healthy tooth as possible, remove caries, reinforce the root with a glass-fiber core to reduce future fracture risk, and finally take impressions.

Final state with zirconia crowns on the two lower left molars.
While extraction followed by implants, bridges, or dentures is common, depending on conditions, teeth can often be preserved.
Although this is private treatment, for those who “cannot accept extraction” or “want to keep teeth as long as possible,” we proactively consider and provide non-extraction care.
Toward Pain-Controlled Dentistry
Many people associate dental care with pain or fear. We strive to make treatment as comfortable as possible.
Once anesthesia is effective, the rest of the procedure is generally painless. However, some discomfort may occur at the moment of injection.
To reduce this, we take several measures to make anesthetic injections less painful.
Topical Anesthesia
The foundation of pain-controlled dentistry is good anesthesia.
Because a needle is used, a brief “prick” is unavoidable.
We apply a gel-type topical anesthetic to numb the surface before injecting.
Ultra-Fine Needles
Thicker needles can cause more pain. We use some of the thinnest needles available in Japan to minimize discomfort.
Warming the Anesthetic
Cold anesthetic can sting more on injection.
We use a dedicated warmer to bring the anesthetic close to body temperature year-round (comfortable even in winter).
Computer-Controlled (Electric) Syringe
Manual injections may cause sudden flow or hand tremor.
Our computer-controlled syringe allows a slow, precise injection rate for comfort and accuracy.
Apical Cysts & Fistulas: Precision Endodontics with a Microscope
Electric NiTi Rotary Files
Among dental procedures, root canal therapy requires particularly fine work.
Tooth roots have complex anatomy; even with CT imaging, there are limits to what the naked eye or tactile sense can achieve.
We therefore utilize a microscope, electric NiTi rotary files, RF devices, and more to improve precision.
These tools enable more precise treatment and minimal removal of tooth structure.
In precision dentistry a microscope is essential; with a Leica® microscope, we perform care beyond what is possible with the naked eye.
We limit caries removal to the minimum necessary, preserving as much natural tooth as possible.
We can also confirm restoration fit in detail, minimizing the “gap between crown and tooth,” which reduces re-do causes and supports long-term tooth survival.
Costs & Insurance Coverage
Treatments such as root-fracture care, intentional replantation, and microscope-assisted precision endodontics may be outside public insurance (private treatment).
Details vary by case, procedure, and site; we explain thoroughly during the initial consultation.
- Initial consultation (counseling): ¥33,000
- Radiographs & CT: included in the consultation
- Root-fracture care including intentional replantation and bone management: approx. ¥330,000–¥880,000 (total)
- Zirconia crown: included in the above totals for private cases
Frequently Asked Questions (FAQ)
Q. Can a tooth told to be extracted really be saved?
A. Depending on the fracture pattern and progression, intentional replantation or adhesive restoration may allow preservation.
After CT and microscopic assessment, we present a treatment plan on the same day.
Note: We often do not perform same-day procedures at the first visit (except urgent trauma such as crown fractures/luxations).
Q. How long does treatment take?
A. It varies by case, root condition, and infection status.
Mild root-level fractures can sometimes be completed in several visits (within ~1 month), whereas cases with periradicular inflammation may require 3–10+ visits over 3–6 months for treatment and follow-up.
Even with severe bone loss, many of our root-fracture cases complete crown delivery in about four months on average.
Q. How is private treatment different from insurance care?
A. Private care allows the use of advanced equipment/materials and longer chair time—often improving long-term maintainability.
We can use regenerative materials, grafts, and precise techniques not typically available under insurance, aiming for higher-precision outcomes.
Q. What kind of patients visit your clinic?
A. Most are from the Kansai region, but some come by car from Hokuriku or Shikoku, and by train from Kanto.
For root-fracture care with intentional replantation, ages range 17–84 (mostly 40s–60s).
By site, fractures are common in maxillary anteriors, maxillary premolars, mandibular molars, maxillary molars, and mandibular premolars; mandibular anterior fractures are relatively rare.
Q. What happens if I leave a fractured tooth untreated?
A. Pain is common initially, but may subside in a few weeks, with many noticing gingival swelling afterward.
Foul odor or pus around the fracture line may cause halitosis.
As supporting bone resorbs, a once partially mobile tooth may become generally mobile.
Long-term neglect risks chronicity and fewer symptoms—please seek evaluation early.
Q. I was told to extract at a university hospital—can it still be okay?
A. Even teeth rejected by several clinics for extraction only may be saved with intentional replantation or adhesive repair.
Many patients who were turned down 3–4 times elsewhere receive satisfactory care here.
Access, Hours, and Appointments
We are located in Minoh, Osaka—about a 5-minute walk from Osaka Metro Midosuji Line “Minoh-Kayano Station.”
We are on the Shin-Midosuji corridor with six parking spaces available.
Hours
Weekdays: 9:00–16:00
Saturday: 9:00–13:00
Closed: Sundays & Public Holidays
If you are visiting from afar, booking in advance helps reduce waiting time.
Please make a reservation by phone (+81-72-725-1182) or via the web form.
Online Reservation